(Educational content onlyno internet links here, but the information reflects established U.S. medical guidance. If you’re noticing new distortion or a dark spot in your central vision, don’t “wait and see” on your ownget a dilated eye exam.)
A macular hole is one of those eye problems that sounds like it should come with a tiny warning label: “May cause straight lines to look like they’re auditioning for a funhouse mirror.” And the tricky part? It often starts subtlyjust enough blur or distortion that you blame lighting, your glasses, or the fact that your phone settings are “definitely weird today.”
The good news is that macular holes are diagnosable with modern retinal imaging and often treatableespecially when caught early. The less fun news is that the fix typically isn’t a new prescription; it’s a very specific plan that may include surgery, a temporary gas bubble in the eye, and (sometimes) the least glamorous yoga pose ever: face-down positioning.
What Exactly Is a Macular Hole?
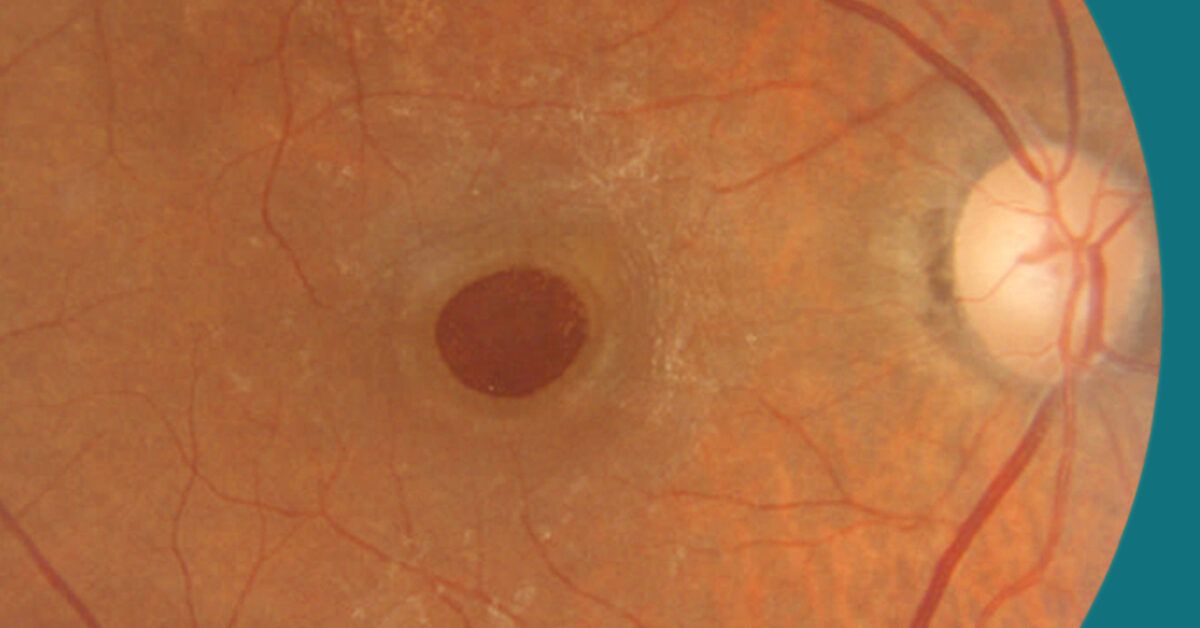
The macula is the center of the retinathe part responsible for crisp, detailed central vision. A macular hole is a defect that forms in that central area. When the hole is “full-thickness,” it means the opening goes through the retinal layers in a way that disrupts fine vision, reading, and recognizing faces.
Importantly, a macular hole is not the same thing as macular degeneration. They can both affect central vision, but they’re different conditions with different treatments. A macular hole is more like a structural “gap” at the fovea (the macula’s sharpest point), whereas age-related macular degeneration involves degenerative changes and, in wet forms, abnormal blood vessels. The symptoms can overlapwhich is why diagnosis matters.
Why Macular Holes Happen: The Vitreous “Tug-of-War”
In many cases, the culprit is vitreous traction. The vitreous is the gel that fills the eye. As we age, that gel naturally changes and can start to separate from the retina. Usually, that separation is uneventful. Sometimes, however, the vitreous holds on a little too tightly at the macula and pulls as it detaches. That pulling can distort the retina and, in some cases, create a hole.
Common risk factors (and why your retina cares)
- Age (macular holes are more common after about age 55–60)
- Sex (many patient resources note a higher frequency in women)
- High myopia (significant nearsightedness can change retinal mechanics)
- Eye inflammation (uveitis) or prior eye conditions affecting the retina
- Trauma (a blow to the eye can trigger a hole, even in younger people)
- Other retinal problems such as macular pucker (epiretinal membrane) or prior retinal detachment
- Diabetic eye disease can also increase risk in some patients
A key clinical reality: if a macular hole develops in one eye, there’s a real (though not guaranteed) chance the other eye could develop one too. That’s one reason retina specialists often recommend monitoring both eyes over time.
Symptoms: The Clues Usually Show Up in the Middle
Macular holes mainly affect central vision. Peripheral vision usually stays intact, which can make the problem feel confusing at firstlike “I can see, but I can’t see.”
Typical symptoms
- Blurred central vision (especially noticeable when reading)
- Distortion (straight lines look bent or wavycalled metamorphopsia)
- A central gray spot or blind spot as the hole progresses
- Trouble with fine detail (threading a needle, reading subtitles, seeing facial features)
A practical example
Imagine reading the word “IMPORTANT” on a pageexcept the “POR” portion looks smudged, warped, or slightly missing. Or you look at your window blinds and one section seems to “kink” like it got a bad haircut. These are classic “central” symptoms that should trigger a real eye exam, not a settings reset.
How Macular Holes Are Diagnosed: The OCT Is the Game-Changer
Diagnosis usually starts with a dilated eye exam. The clinician examines the retina directly and assesses for changes at the macula. But the modern workhorse for macular holes is optical coherence tomography (OCT)a fast, noninvasive imaging test that creates a cross-sectional “slice” view of the retina.
OCT helps clinicians:
- Confirm whether the defect is a full-thickness macular hole or something similar-looking
- Measure size and stage (small/medium/large by minimum diameter is commonly described)
- See if there’s vitreomacular traction actively pulling
- Track healing after treatment
Why “similar-looking” matters
Several conditions can mimic macular-hole symptoms. OCT helps differentiate:
- Lamellar macular hole (partial-thickness defect)
- Macular pseudohole (often from an epiretinal membrane, with steep edges but no true tissue loss)
- Epiretinal membrane (macular pucker) causing wrinkling and distortion
- Wet AMD or other macular diseases
This distinction is not academic nitpickingit changes the plan. Treating the wrong “hole” is like fixing a leaky faucet by repainting the wall.
Do Macular Holes Ever Heal on Their Own?
Sometimes. Very early or small holesor situations where traction is mild and resolvesmay be monitored. Retina specialists might recommend watchful waiting when the hole is tiny and symptoms are minimal, because there are cases where early-stage changes improve without surgery.
That said, a confirmed, symptomatic full-thickness macular hole often needs active treatment to maximize the chance of closure and meaningful vision recovery. Timing can matter: in general, smaller and more recent holes tend to have better outcomes.
Treatment: From “Let’s Watch” to “Let’s Fix This”
1) Vitrectomy: The main event
The most common treatment is pars plana vitrectomy performed by a retina specialist. In plain English: the surgeon removes the vitreous gel so it can’t keep tugging on the macula.
Many macular hole repairs also include peeling the internal limiting membrane (ILM), a thin surface layer of the retina. Removing it reduces traction and can improve the odds that the hole seals.
2) The gas bubble: your temporary “internal Band-Aid”
After the vitreous is removed and the area is stabilized, surgeons commonly place a gas bubble inside the eye. The bubble helps press the edges of the hole into position while the retina heals. Over time, the bubble dissolves and is replaced by the eye’s natural fluid.
While the bubble is present, vision in that eye may be quite blurrymany people describe it as looking through water, fog, or a shifting level line. That can be normal during recovery, even though it’s annoying and makes reading with that eye basically a nonstarter for a bit.
3) Face-down positioning: sometimes required, sometimes reduced
You may be asked to keep your head positioned in a way that holds the bubble against the macula. For some patients, that means face-down positioning for several days (and occasionally longer, depending on the hole and surgical approach). Some surgeons reduce or eliminate strict face-down instructions in selected cases, but positioning recommendations are individualized.
Translation: your retina surgeon is not trying to ruin your week. They’re trying to get the physics right.
4) Options for “big” or stubborn holes
Larger, chronic, highly myopic, or previously repaired-but-reopened holes may require more advanced techniques. Surgeons sometimes use variations of ILM flap methods (rather than a standard peel) to provide a scaffold that supports closure. These approaches are part of how modern retina surgery has improved closure rates for challenging cases.
5) Medication injection (selected cases)
In some situations, a medication injection aimed at relieving vitreous traction (such as ocriplasmin) may be discussed. It isn’t the main approach for most patients, but it can appear on the menu depending on the exact anatomy and traction.
Recovery: What “Normal” Can Look Like After Repair
Recovery is rarely instant. Even if the hole closes promptly, the brain and retina may take time to “re-learn” crisp detail. Many patients notice gradual improvement over weeks to months.
Common recovery expectations
- Blurry vision while the bubble is present (the bubble may last weeks, depending on the gas used)
- Activity restrictions as advised by your surgeon
- No flying or high-altitude travel while a gas bubble is in the eye (air pressure changes can be dangerous)
- Eye drops to reduce infection risk and inflammation
- Follow-up visits to confirm closure (often with OCT)
One extremely practical tip: if you have a gas bubble, tell every medical provider you seeespecially if you need surgery or anesthesia. Certain anesthetic gases can interact dangerously with an intraocular gas bubble.
Results and Prognosis: How Successful Is Treatment?
For many typical (idiopathic) macular holes treated with vitrectomy, reported closure rates are commonly above 90%. Vision often improves, but the amount of improvement varies with:
- Size of the hole
- How long it has been present
- Stage and retinal health
- Other eye diseases (like significant diabetic retinopathy or high myopia changes)
It’s also normal for vision to improve without returning to “factory settings.” Many people regain functional central vision for reading and daily tasks, even if fine print still needs help.
Risks: The Part No One Likes, but Everyone Should Understand
Macular hole surgery is generally considered safe and effective, but it is still surgery. Potential complications can include:
- Cataract progression (very common after vitrectomy in people who still have their natural lens)
- Retinal detachment
- Infection (rare but serious)
- Bleeding
- Elevated eye pressure (glaucoma-related issues)
- Hole persistence or reopening, sometimes requiring additional treatment
Your surgeon will weigh these risks against the risk of leaving the hole untreated, which can include enlargement and permanent central vision loss.
Macular Hole vs. “Other Stuff That Makes Lines Wavy”
Distortion isn’t exclusive to macular holes. A few common lookalikes:
- Epiretinal membrane (macular pucker): scar-like tissue that wrinkles the macula
- Vitreomacular traction (VMT): traction without a full-thickness hole
- Wet AMD: can distort central vision and create gray spots
- Central serous chorioretinopathy: can cause blurry central spots
This is why OCT is so valuable. It turns “maybe” into a clearly mapped plan.
Real-World Experiences (500+ Words): What Patients Commonly Describe
The stories below are composite experiences drawn from common patient reports and typical clinic conversationsnot specific individuals. They’re included because macular hole treatment is not just anatomy and acronyms; it’s also a very human “how do I live my life while my eye heals?” situation.
Experience #1: “I Thought It Was My Glasses… Then the Doorframe Bent”
A lot of people describe the beginning as weirdly easy to dismiss. One eye still sees well, so your brain quietly “fills in the gap.” You might notice that letters look slightly warpedlike they’ve been italicized by a mischievous graphic designer. A classic moment is realizing that straight lines aren’t straight: the edge of a doorframe bows, the grout lines in a bathroom tile look rippled, or the lines on a spreadsheet (cruel irony) develop a kink right in the center.
People often test themselves without realizing it: “If I cover my left eye, is it still happening?” That simple cover-one-eye check is a big deal, because macular holes are frequently one-eye problems at first. Many patients say the appointment happened because the distortion stopped being “occasionally annoying” and became “okay, this is messing with reading and driving signs.”
Experience #2: The OCT Moment“So That’s What My Retina Looks Like”
OCT imaging can be oddly reassuring. Patients often describe it like seeing a weather radar for the eye: suddenly the doctor can point to the exact location of the problem and explain why symptoms feel so specific. It’s also a moment where people realize this isn’t something you “eyedrop” away. That clarity helps with decision-making: watching a very small or early change can feel reasonable, while a true full-thickness hole usually shifts the conversation toward repair.
A common emotional arc is: relief that it’s diagnosable, concern that it may need surgery, and then comfort when the surgeon explains how routine macular hole repair has become for retina teams.
Experience #3: Life With a Gas Bubble“I’m Staring at a Floating Horizon Line”
After surgery, the gas bubble becomes the star of the show. People describe it as a moving line across visionlike having a tiny level tool inside the eye. As it shrinks, that line drops lower and lower, sometimes creating a fun (and distracting) sensation that you’re watching your vision “refill.” Many patients are surprised by how blurry the operated eye is early on, especially if they expected immediate improvement. Clinics usually warn about this, but living it is different than hearing it.
Another frequent experience: depth perception feels off for a while, particularly if the other eye isn’t perfect either. People become very aware of curbs, stairs, and pouring coffee without missing the mug (a heroic daily quest). Most adapt by improving lighting, using larger text, and leaning on the stronger eyetemporarily.
Experience #4: Face-Down PositioningA Surprisingly Creative Time
If face-down positioning is recommended, it can feel like a full-time job with zero benefits and terrible office chairs. Patients get creative: massage tables, specialized positioning equipment, stacks of pillows engineered like a NASA launch pad, and audiobook libraries that suddenly expand by 40 titles.
The most common advice people wish they’d heard earlier is simple: plan support. Arrange meals, rides, and “easy wins” entertainment before surgery. It’s also normal to feel cranky during positioningyour neck, back, and patience are doing the heavy lifting. The bright side is that many patients say the discomfort felt worth it once follow-up imaging confirmed closure.
Experience #5: The Slow-But-Real Improvement
When the bubble finally goes away, many people describe a moment of “Oh! There’s the world again,” followed by gradual sharpening. Reading may still require larger print at first, and distortion can fade slowly. Some patients notice that faces look less “smudged,” subtitles become readable again, or the center of vision feels less washed out. The key theme is patience: macular healing and visual recovery are often measured in weeks to months, not days.
Conclusion
Macular holes are tricky because they can start quietly and masquerade as everyday vision annoyances. But they’re also one of the more “fixable” macular problems when properly diagnosedespecially with OCT imaging guiding the plan. Whether your best path is monitoring a tiny early change or moving forward with vitrectomy and a gas bubble, the biggest advantage you can give your future vision is simple: don’t delay evaluation when distortion shows up.
