Low AMH levels can feel like receiving a sternly worded email from your ovaries: “We need to talk.” But before you spiral into late-night search results and suspicious supplement ads, take a breath. Anti-Müllerian hormone, or AMH, is a blood marker that helps estimate ovarian reservethe approximate number of eggs remaining. It does not perfectly measure egg quality, guarantee infertility, or predict your future with the confidence of a fortune cookie wearing a lab coat.
The phrase “treat low AMH levels” needs careful framing. In most cases, the goal is not to magically refill the ovarian reserve. Biology is not a printer cartridge. Instead, treatment means understanding why AMH is low, protecting fertility where possible, improving overall reproductive health, and choosing the smartest path toward pregnancy if that is your goal.
This guide explains 12 practical, evidence-aligned ways to respond to low AMH levels, from fertility testing and lifestyle changes to IVF planning, supplements, and emotional support. The aim is simple: less panic, more strategy.
What Does Low AMH Mean?
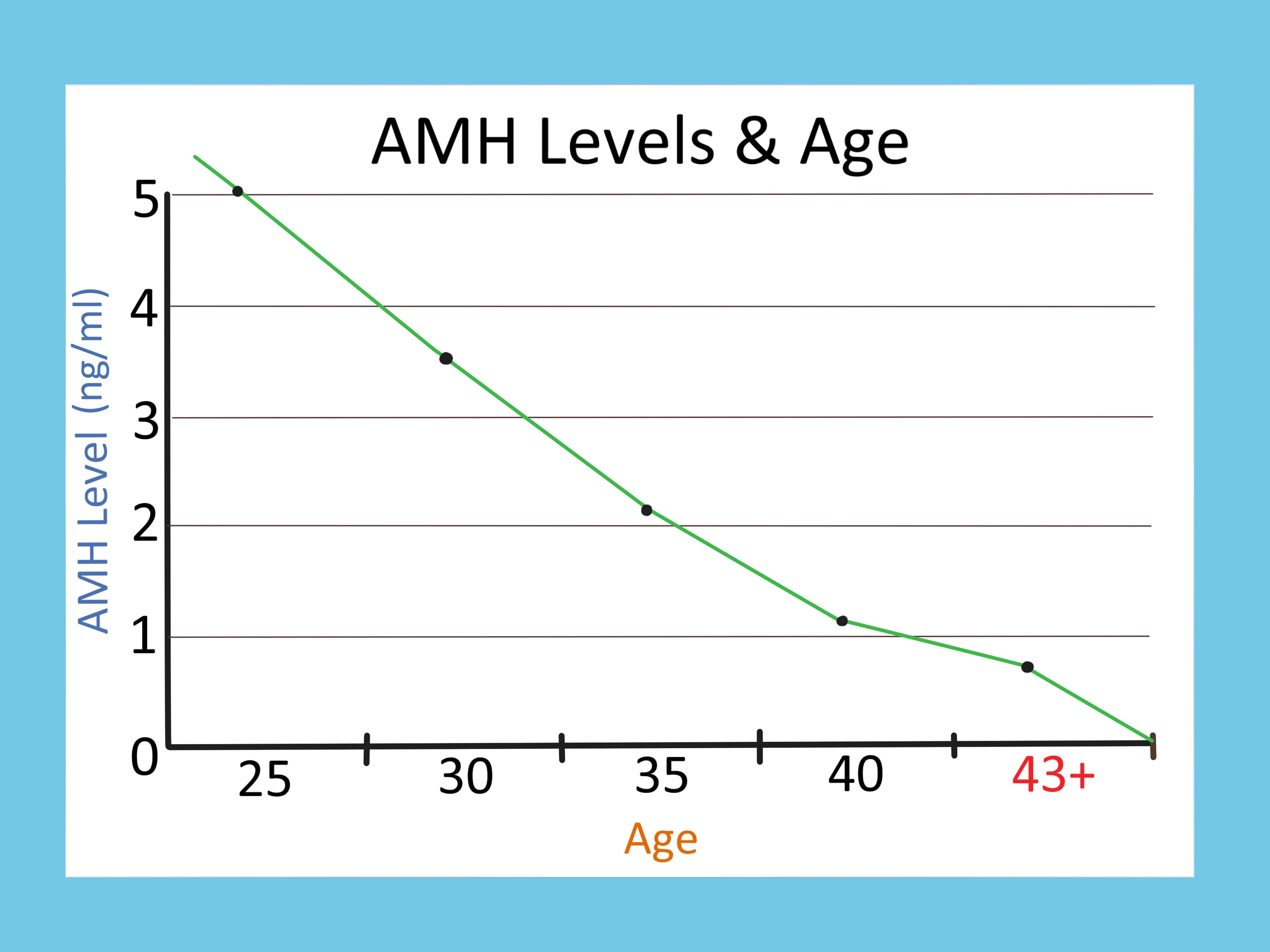
AMH is produced by small follicles in the ovaries. A lower AMH level may suggest fewer recruitable follicles compared with what is typical for your age. Doctors often use AMH alongside other information, such as antral follicle count, follicle-stimulating hormone, estradiol, menstrual history, age, and ultrasound findings.
Low AMH is commonly associated with diminished ovarian reserve. However, it is not the whole fertility story. Age remains one of the biggest factors because egg quality usually declines over time. A younger person with low AMH may still have better egg quality than an older person with a higher AMH. In other words, AMH is important, but it is not the main character in every scene.
1. Confirm the Result Before Making Big Decisions
The first way to treat low AMH levels is to make sure the result is meaningful. AMH testing can vary by lab, assay, timing, birth control use, medical history, and individual biology. A single result should not be treated like a final judgment.
What to do next
Ask your doctor whether you should repeat the AMH test, especially if the result does not match your age, cycle pattern, or ultrasound findings. Request a full fertility workup if you are trying to conceive. This may include antral follicle count, FSH, estradiol, thyroid testing, prolactin, ovulation tracking, uterine evaluation, fallopian tube testing, and semen analysis for a partner if relevant.
Low AMH can be stressful, but clear information is calming. Think of testing as turning on the lights in a messy room. The room may still be messy, but at least you stop stepping on emotional Legos.
2. See a Reproductive Endocrinologist Early
If you have low AMH and want to become pregnant now or in the future, consider meeting with a reproductive endocrinologist. This is especially important if you are 35 or older, have irregular periods, have a history of ovarian surgery, endometriosis, chemotherapy, radiation, autoimmune conditions, or have been trying to conceive without success.
Why timing matters
Low AMH may mean fewer eggs are likely to respond during ovarian stimulation. A fertility specialist can help you decide whether to keep trying naturally, move to intrauterine insemination, consider IVF, freeze eggs or embryos, or explore donor eggs. Earlier planning often gives you more options.
This does not mean everyone with low AMH needs aggressive treatment immediately. It means you deserve a plan based on your actual situation rather than a random internet comment from someone named “BabyDustQueen92.”
3. Treat Underlying Health Conditions
Low AMH may be related to age, genetics, prior ovarian surgery, endometriosis, chemotherapy, radiation, autoimmune disease, or unknown factors. While not every cause can be reversed, some related conditions can be managed to improve the overall fertility environment.
Conditions worth discussing
Ask your clinician about thyroid disease, vitamin D deficiency, endometriosis, pelvic infections, autoimmune disorders, diabetes, insulin resistance, and menstrual irregularities. These issues may not “raise AMH” in a dramatic way, but managing them can support ovulation, implantation, pregnancy health, and treatment readiness.
The goal is not to chase a prettier lab number. The goal is to improve the whole reproductive system’s working conditions. Ovaries, like office employees, perform better when the environment is not chaotic.
4. Stop Smoking and Avoid Tobacco Exposure
If there is one lifestyle step with a strong fertility argument, it is quitting tobacco. Smoking is associated with reduced ovarian reserve and poorer fertility treatment outcomes. It may also affect egg quality, miscarriage risk, and the timing of menopause.
Practical steps
Ask your doctor about smoking cessation support, nicotine replacement options, counseling, and prescription medications if appropriate. Avoid vaping and secondhand smoke when possible. If quitting feels hard, that is not a personal failure. Nicotine is addictive; getting help is smart, not weak.
This is one of the few changes that can help your fertility, lungs, heart, skin, wallet, and laundry smell all at once. Very few health interventions are that overachieving.
5. Build a Fertility-Supportive Diet
No diet has been proven to restore ovarian reserve, but nutrition can support hormone balance, inflammation control, energy, and pregnancy readiness. A fertility-supportive eating pattern usually looks a lot like a heart-healthy Mediterranean-style diet.
What to include
Focus on vegetables, fruits, beans, lentils, whole grains, nuts, seeds, olive oil, fish rich in omega-3 fats, eggs, yogurt, and lean proteins. Choose high-fiber carbohydrates and limit ultra-processed foods, trans fats, and sugary drinks. If you eat vegetarian or vegan, pay attention to iron, B12, iodine, zinc, omega-3s, calcium, and protein.
For example, a fertility-friendly lunch might be salmon or chickpeas over quinoa with spinach, avocado, tomatoes, olive oil, and lemon. Is it a magic AMH bowl? No. Is it a good idea for your body? Absolutely.
6. Aim for a Healthy Weight Without Crash Dieting
Both undernutrition and excess body fat can interfere with ovulation, inflammation, insulin sensitivity, and treatment outcomes. However, extreme dieting can also disrupt cycles and increase stress. The goal is not to shrink yourself into fertility. The goal is metabolic stability.
Balanced approach
If weight is a concern, work with a doctor or registered dietitian. A modest, sustainable change in nutrition, movement, and sleep can be more helpful than a dramatic crash diet. For people with insulin resistance or polycystic ovary syndrome, personalized metabolic care may be especially important.
Low AMH already brings enough pressure. You do not need a diet plan that makes you fear bananas. Choose steady habits over punishment.
7. Consider CoQ10, Vitamin D, and Prenatal Nutrients Carefully
Many people with low AMH search for supplements that promise better egg health. Some supplements are biologically plausible, but evidence varies, and more is not always better.
Common options to discuss with your doctor
Coenzyme Q10 is often discussed for egg quality because it plays a role in mitochondrial function. Vitamin D may be checked because deficiency is common and may be linked with reproductive health markers, although research on AMH changes is mixed. A prenatal vitamin with folic acid or folate is generally recommended before pregnancy to reduce the risk of neural tube defects.
Do not take high-dose supplements without medical guidance. Supplements can interact with medications, affect hormone-sensitive conditions, and vary in quality. Look for third-party testing when possible. The fertility aisle can be expensive, emotionally persuasive, and occasionally as scientifically stable as a folding chair at a family reunion.
8. Be Cautious With DHEA and Hormone-Based Supplements
DHEA is sometimes suggested for diminished ovarian reserve or poor ovarian response, especially before IVF. Some studies suggest possible benefits in selected patients, while other reviews and expert opinions remain cautious. DHEA can affect androgen and estrogen levels and may cause acne, oily skin, hair growth, mood changes, or other side effects.
Safe use matters
If you are considering DHEA, do it only under the supervision of a reproductive endocrinologist. Your clinician may check androgen levels, review your medical history, and decide whether it makes sense for your specific diagnosis. It is not suitable for everyone, especially people with hormone-sensitive conditions or certain metabolic risks.
The rule is simple: if a supplement acts like a hormone, treat it with the respect you would give a tiny, unlicensed endocrinologist in a bottle.
9. Choose the Right Fertility Treatment Strategy
Low AMH often matters most when planning fertility treatment because it may predict a lower response to ovarian stimulation. That means fewer eggs may be retrieved in an IVF cycle. But fewer eggs does not mean zero chance.
Possible treatment paths
Your doctor may discuss timed intercourse, ovulation induction, IUI, IVF, embryo banking, egg freezing, or donor eggs. IVF protocols may be adjusted with different medication doses, stimulation approaches, trigger strategies, or embryo-freezing plans. Some patients may need more than one cycle to collect enough eggs or embryos.
The best plan depends on age, AMH, antral follicle count, sperm factors, fallopian tube status, pregnancy history, budget, emotional bandwidth, and family-building goals. Fertility treatment is not one-size-fits-all. It is more like tailoring jeans: the right fit matters, and nobody enjoys the process under fluorescent lights.
10. Consider Egg or Embryo Freezing If Pregnancy Is Not Immediate
If you are not ready to become pregnant but know you want children later, low AMH may be a reason to discuss fertility preservation sooner rather than later. Egg freezing or embryo freezing can be useful options, although success depends heavily on age and the number of eggs retrieved.
Questions to ask
Ask how many eggs your doctor estimates you may retrieve per cycle, how many cycles might be needed, what the costs include, and what success rates look like for your age group. If you have a partner or want to use donor sperm, embryo freezing may be discussed because embryos provide more information about fertilization and development than eggs alone.
Freezing eggs is not a guarantee. It is more like buying insurance: helpful for some people, imperfect, and definitely worth reading the fine print before signing.
11. Reduce Environmental and Medical Risks Where Possible
You cannot control every factor affecting ovarian reserve, but you can reduce avoidable reproductive stressors. This includes avoiding tobacco, limiting heavy alcohol intake, minimizing exposure to endocrine-disrupting chemicals when practical, and discussing fertility protection before surgeries or treatments that may affect the ovaries.
Smart prevention
If you need ovarian surgery for cysts or endometriosis, ask how the procedure may affect ovarian reserve and whether fertility preservation should be considered first. If you are facing chemotherapy or radiation, ask urgently about egg or embryo freezing before treatment begins, if time allows.
At home, you do not need to live in a bubble. Simple steps like not microwaving food in old plastic containers, choosing fragrance-free products when possible, and washing produce can be reasonable. Fertility care should improve your life, not turn you into a detective yelling at receipts.
12. Protect Your Mental Health During the Process
Low AMH can trigger grief, anxiety, anger, and a strange obsession with lab portals. That emotional response is valid. Fertility uncertainty is not just a medical issue; it touches identity, relationships, finances, timelines, and hope.
Support that helps
Consider therapy, fertility counseling, support groups, journaling, mindfulness, gentle exercise, or honest conversations with trusted people. If you are partnered, schedule fertility-free time where you talk about anything except ovulation, insurance, injections, and whether the clinic called back.
Mental health support will not raise AMH like a thermostat. But it can help you make decisions from a steadier place. And in fertility care, steadier is powerful.
When Should You Seek Help for Low AMH?
Talk with a healthcare provider if you have low AMH and are trying to conceive, planning future pregnancy, have irregular cycles, are over 35, have a history of endometriosis or ovarian surgery, or have been exposed to chemotherapy or radiation. If you are under 35 and have tried to conceive for 12 months, or 35 or older and have tried for six months, fertility evaluation is usually recommended. Seek help sooner if you already know there may be a fertility issue.
Bring your test results, cycle history, medication list, supplement list, and questions. Ask what your AMH means for your age, how it compares with your antral follicle count, and what options match your goals. A good fertility visit should leave you with a plan, not just a new collection of acronyms.
Can Low AMH Be Reversed?
In most cases, low AMH cannot be truly reversed because it reflects the remaining pool of eggs. Some factors may temporarily affect AMH readings, and treating deficiencies or health problems may improve reproductive health. But no diet, supplement, injection, or “ovary detox tea” has been proven to create new eggs or restore ovarian reserve to a younger state.
That may sound discouraging, but there is a more hopeful interpretation: you do not need to waste precious time chasing fake cures. You can focus on the strategies most likely to helpaccurate diagnosis, timely treatment, healthy habits, fertility preservation, and emotionally sustainable decision-making.
Personal Experiences and Real-World Lessons About Low AMH
Many people describe the moment they learn they have low AMH as strangely quiet. The doctor may explain the result calmly, but the brain hears one thing: “time.” Suddenly every birthday feels louder, every pregnancy announcement lands differently, and every supplement advertisement seems to know exactly where the emotional bruise is. This is one reason low AMH deserves compassionate care, not just clinical interpretation.
One common experience is confusion. A person may have regular periods, feel healthy, exercise often, and assume everything is working normally. Then AMH comes back low, and the result feels incompatible with daily life. This is because AMH does not always announce itself through obvious symptoms. You can have predictable cycles and still have a lower ovarian reserve than expected for your age. That mismatch can feel unfair, but it is also why a full evaluation matters.
Another real-world lesson is that couples often discover low AMH while investigating something else. Sometimes the original issue is male-factor infertility, irregular ovulation, recurrent pregnancy loss, or simply “we have been trying and nothing is happening.” Then low AMH appears in the workup and steals the spotlight. A good fertility specialist helps put it back in context. Low AMH is important, but it should not erase other diagnoses or make every decision automatic.
People who go through IVF with low AMH often learn to measure progress differently. Someone with high ovarian reserve may retrieve many eggs in one cycle. Someone with low AMH may retrieve fewer, and every follicle can feel emotionally significant. The waiting periodswaiting for follicles to grow, eggs to fertilize, embryos to develop, genetic testing results, transfer daycan feel like a long obstacle course designed by someone with no respect for human nerves.
Yet many patients also describe becoming more informed and confident over time. They learn what questions to ask: What is my antral follicle count? Is my protocol personalized? Should we consider embryo banking? What are realistic success rates for my age? Are supplements appropriate for me? Should we move faster? Should we pause? The first appointment may feel overwhelming, but the second or third often feels more manageable because knowledge replaces some of the fog.
There is also an emotional lesson about comparison. Fertility forums can be helpful, but they can also become a carnival of numbers: AMH, FSH, AFC, eggs retrieved, embryos frozen, beta levels. These numbers matter, but they are not a moral score. A low AMH result does not mean someone waited too long, failed their body, or made bad choices. Biology is complex, and blame is not treatment.
The most helpful experiences often involve building a support system. That may include a reproductive endocrinologist, OB-GYN, therapist, dietitian, acupuncturist, partner, friend, or support group. The best support people do not offer miracle cures or say, “Just relax.” They say, “I am here. What do you need today?” Sometimes the answer is research help. Sometimes it is a ride home from retrieval. Sometimes it is tacos and silence.
Ultimately, living with low AMH is about making informed choices under imperfect conditions. It requires urgency without panic, hope without denial, and realism without cruelty. The number matters, but it is not the whole story. You are allowed to feel scared. You are also allowed to ask for options, second opinions, and care that treats you like a personnot a lab value with shoes.
Conclusion
Low AMH levels can be emotionally overwhelming, but they are not a final verdict. AMH is a useful marker of ovarian reserve and potential response to fertility medication, but it does not fully predict egg quality, natural conception, or your worth as a future parent. The best approach is strategic: confirm the result, get a complete fertility evaluation, consult a reproductive endocrinologist, manage underlying health conditions, stop smoking, support your body with nutrition and sleep, use supplements carefully, and consider fertility treatment or preservation when appropriate.
The most important takeaway is this: do not spend months chasing miracle AMH cures while missing the opportunity to make a real plan. Low AMH calls for clear information, timely action, and compassionate support. Your ovaries may be giving you data, but your next steps should come from evidence, expert guidance, and your personal goalsnot fear.
Note: This article is for educational purposes only and is not a substitute for medical diagnosis or treatment. Anyone with low AMH levels, infertility concerns, irregular periods, or plans for pregnancy should consult a qualified healthcare provider or reproductive endocrinologist.